by Roseann Vorce, Ph.D.,
Department of Pharmacology and Toxicology, Michigan State University
If you’ve noticed the headlines, and they’ve been almost impossible to miss, you’ve probably wondered how HIV researchers cured an HIV-infected infant.
- “Baby Cured of HIV for the First Time, Researchers Say” (Wall Street Journal)
- “Baby cured of HIV offers hope” (USA Today)
- “US doctors cure child born with HIV” (The Guardian, UK)
- “Baby’s HIV “cure” differs from previously reported case” (CBS News)
These headlines are based on a paper presented at the 20th Conference on Retroviruses and Opportunistic Infections. According to the report, physicians effected a functional cure of an HIV-infected infant using aggressive antiretroviral drug therapy initiated shortly after birth. This news is exciting because this baby is the first person to have been cured of HIV through drug therapy. Although you might suspect that a novel anti-HIV drug was responsible for the baby’s cure, she was initially treated with three standard antiretroviral drugs: zidovudine, lamivudine, and nevirapine.
Before we take a closer look at the case of the groundbreaking cure, let’s examine the three drugs used in this patient.
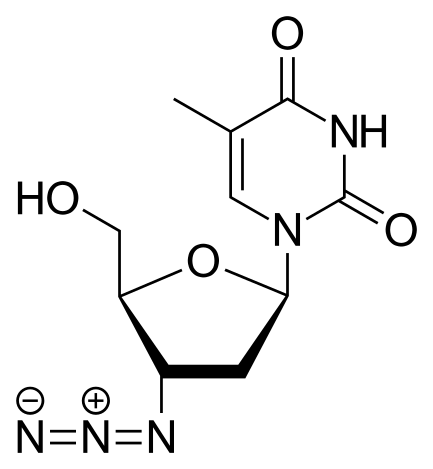
Zidovudine
Zidovudine, lamivudine, and nevirapine all inhibit the HIV enzyme reverse transcriptase (RT). This enzyme converts viral RNA into DNA, and inhibition of RT inhibits HIV replication. By combining drugs that use complementary mechanisms to inhibit RT activity, physicians have been able to dramatically decrease the viral load in HIV positive patients. However, this drug combination has never before eliminated HIV from an infected person.
Zidovudine (AZT) competitively inhibits RT because this drug is an analog of thymidine. When RT incorporates a zidovudine molecule into the newly synthesized DNA strand, chain elongation is terminated, and an incomplete DNA molecule is produced. Similarly, lamivudine inhibits RT because this drug is an analog of deoxycytidine. DNA chain elongation is blocked when RT incorporates a lamivudine molecule into DNA, again producing an incomplete DNA molecule. Due to its rapid mutation rate, HIV readily develops resistance to both zidovudine and lamivudine. However, the RT gene only rarely acquires mutations that confer resistance to both drugs. Therefore, simultaneous administration of these two competitive inhibitors inhibits HIV replication and delays the development of resistance, resulting in a decreased viral load in HIV positive patients.
Lamivudine
Zidovudine and lamivudine are nucleoside prodrugs that are well-absorbed after oral administration. Both drugs readily cross cell membranes to reach the intracellular compartment. Once drug molecules reach the inside of a cell, they are phosphorylated to the triphosphate form, which is the active form of the drugs. In addition to serving as the active drug species, the phosphorylated forms of zidovudine and lamivudine cannot diffuse back through the cell membranes; in essence, phosphorylation traps the drug at its site of action within cells. For this reason, zidovudine and lamivudine remain active even after plasma drug levels have fallen dramatically. Therefore, once daily dosing produces adequate pharmacological activity.
The third drug, nevirapine, also inhibits RT activity, but this non-nucleoside RT inhibitor uses a different mechanism. Instead of competing with wild type nucleotides for the catalytic binding site, nevirapine binds to a separate allosteric binding site on RT. Upon binding, nevirapine alters the conformation of the catalytic site of the enzyme, thereby inactivating it. After oral administration, nevirapine exhibits good bioavailability and readily penetrates the cell membrane. The cytochrome P450 system metabolizes this drug to produce several metabolites, which are subsequently glucuronidated and excreted in urine. Nevirapine induces its own metabolism, requiring patients to increase the dose after two weeks on the drug. HIV readily develops resistance to nevirapine, and co-administration of this drug with other RT inhibitors improves efficacy and inhibits the emergence of drug-resistant strains.

Nevirapine
Now that we know which drugs were used, let’s return to the baby girl who was cured of HIV.
She was born to an undiagnosed and untreated HIV positive mother. Consequently, she was treated almost immediately with an aggressive regimen of zidovudine, lamivudine, and nevirapine. A week later, the combination of lopinavir (inhibits HIV protease) and ritonavir (inhibits the P450 that metabolizes lopinavir) replaced the nevirapine. After 18 months of treatment, therapy was discontinued. Because cessation of drug therapy typically causes the retroviral load to rebound, HIV researchers were elated that the child tested negative several months later! Using ultrasensitive methods to detect HIV RNA, researchers found a vanishingly small number of RNA copies, but they detected no replication competent virus. Therefore, the initial therapy appears to have cured this child of HIV infection, and she remains HIV negative.
If the drugs used to treat the infant weren’t new, then what was the difference responsible for the functional cure? The simple answer is that the physicians initiated therapy using an aggressive treatment protocol in lieu of a more conservative prophylaxis protocol. Instead of administering one or two RT inhibitors to prevent the baby from becoming infected, doctors administered all three RT inhibitors starting almost immediately (31 hours after birth). This treatment protocol was initiated because the mother had not received prenatal care designed to minimize transmission of HIV to the infant. When the mother’s positive HIV status is known in advance, she receives anti-HIV therapy during pregnancy, which dramatically decreases the infant’s infection rate. In addition, the infant is treated with a postnatal drug regimen designed to prevent infection. In this case, the mother received no prenatal care, and her positive HIV status was not discovered until she was in labor. The physicians’ decision to treat the baby aggressively paid off: tests confirmed that she had been infected prior to birth, and the treatment regimen has produced a functional cure of her HIV infection.
Although some scientists have suggested that the infant was not truly infected, the fact remains that the baby tested HIV-positive shortly after birth, responded in a typical fashion to antiretroviral therapy, received treatment for only 18 months, and has tested negative from ages 24-26 months. This unprecedented finding suggests that a functional cure of HIV infection is within our grasp, if the right combination of antiretroviral drugs is administered at the right time and at the right doses. This report also demonstrates that scientific progress often occurs incrementally, using known tools in a different way, administering standard drugs using a different protocol, or by a physician violating standard treatment protocol when the conditions surrounding patient care are not standard.
————–
References:
Persaud D, Gay H, Ziemniak C, Chen YH, Piatak M, Chun T-W, Strain M, Richman D, and Luzuriaga K. Functional HIV cure after very early ART of an infected infant. 20th Conference on Retroviruses and Opportunistic Infections, Paper #48LB, 2013. Accessed on 06 March 2013 from: http://www.retroconference.org/2013b/Abstracts/47897.htm
http://www.niaid.nih.gov/news/newsreleases/2013/Pages/toddlerfunctionallycured.aspx

March 7, 2013 at 9:39 pm
Wonderful and amazing!! Any word of cures for ms??
Thank You
March 8, 2013 at 9:42 pm
It is a wonder discovery. This will endorse many researchers accross the globe.
March 11, 2013 at 2:23 pm
Intellectually analyzed and thoughtful insight.Exciting to have this break through and hope for the future but more time should still be given before a final conclusion can be made considering the variance in mutaton exhibited by viruses and presence of varnishinly small copies of HIV RNA still present furthermore knowing the reserviors are in the macrophages.A protocol review being made to follow this new trend I believe will impact similarly infected circumstantial populace.